I decided to make a post on this topic after seeing the popular press articles about a study claiming reversal of human biological (as opposed to chronological) aging. That study used human growth hormone (HGH), DHEA and metformin combination as an intervention that restores thymus health and thus reverses immunosenescence (immune system aging). It is well-known in medical circles that the so-called “thymus involution” (atrophy) is a major cause of both morbidity and mortality in aging humans and is a major factor in increased risk for both infectious and chronic diseases such as diabetes, cancer, dementias, CVD, etc. As such, multiple (animal) studies have shown that reversing thymus atrophy/involution has been shown to have strong protective effects from the so-called “age-related diseases”.
First, the good news. The study noted that as a result of the 12-month treatment, on average there was about 2.5 years of biological age reversal for the participants. Moreover, the reversal of biological age markers accelerated after about 9 months of treatment and over the last 3 months of treatment averaged about 6.48 years / year of biological age reversal. Not bad at all! Especially considering we have been told repeatedly that aging is a “natural” process, is not a disease, and cannot be reversed.
https://www.nature.com/articles/d41586-019-02638-w
“…A small clinical study in California has suggested for the first time that it might be possible to reverse the body’s epigenetic clock, which measures a person’s biological age. For one year, nine healthy volunteers took a cocktail of three common drugs — growth hormone and two diabetes medications — and on average shed 2.5 years of their biological ages, measured by analysing marks on a person’s genomes. The participants’ immune systems also showed signs of rejuvenation. The results were a surprise even to the trial organizers — but researchers caution that the findings are preliminary because the trial was small and did not include a control arm. “I’d expected to see slowing down of the clock, but not a reversal,” says geneticist Steve Horvath at the University of California, Los Angeles, who conducted the epigenetic analysis. “That felt kind of futuristic.” The findings were published on 5 September in Aging Cell.”
https://www.gwern.net/docs/longevity/2019-fahy.pdf
“…Furthermore, comparing the rates of aging regression between 0–9 and 9–12 months showed that, for every age estimator, the rate of aging regression appeared to accelerate substantially with increasing treatment time (Figure 5a–d and Table 1), with a mean slope over all four clocks of −1.56 ± 0.46 years/year in the first 9 months to −6.48 ± 0.34 years/year in the last 3 months of treatment (p < .005, Figure 5f).”
OK, so what is the bad news? Well, the trial design is bizarre, unsafe and likely purposefully biased. It ignores both the risks of its interventions as well as opportunities to achieve much more striking reversals of biological aging using other interventions. I highly doubt that the trial designers are stupid, so I suspect something more sinister is at play here (as I explain below). The first bizarre and unsafe intervention is HGH. As the study above notes, HGH was used because of its purported rejuvenating effects on the thymus. Why bizarre? Well, as the study itself states HGH has a known potent diabetogenic effect. Moreover, as the study itself states, HGH can actually have pro-aging effects on thymus and immune system.
“…Because GH‐induced hyperinsulinemia (Marcus et al., 1990) is undesirable and might affect thymic regeneration and immunological reconstitution, we combined rhGH with both dehydroepiandrosterone (DHEA) and metformin in an attempt to limit the “diabetogenic” effect of GH (Fahy, 2003, 2010; Weiss, Villareal, Fontana, Han, & Holloszy, 2011).”
So, let me get this straight. The main intervention in the trial not only may cause diabetes (which itself has a VERY close association with aging) but can actually have pro-aging effects on both thymus and immune system in general! Wait, don’t take my word for it, the pro-aging and mortality-increasing effects of HGH have already been confirmed in humans, while its purported anti-aging effects appear to be based on nothing but overhyping of a single study, that even its own authors did not think demonstrated anti-aging effects of HGH.
https://www.livescience.com/44436-anti-aging-hormone-may-actually-shorten-life.html
“…Call it anti-anti-aging therapy. It turns out that injections of growth hormone — a staple of anti-aging, hormone-replacement therapy — may have the opposite effect as intended, thwarting a person’s quest to live to an advanced age. In an ongoing study of very old people, those in their 90s with naturally low levels of human growth hormone appear to have a far better chance of living into their 100s compared with people who have above-average levels of the hormone. In other words, juicing yourself up with growth hormones as an anti-aging strategy might backfire, undermining the body’s natural defenses against the diseases of old age, according to researchers at Albert Einstein College of Medicine in New York. Their study appears in the April issue of the journal Aging Cell.”
“…This industry traces its roots to a 1990 New England Journal of Medicine study, in which 12 men over age 60 were given shots of growth hormone. The men experienced a modest increase in muscle mass and bone density, and a decline in body fat. To some entrepreneurs, that meant “anti-aging,” and they have repackaged the study that way ever since. But the treatment came with side effects and myriad unknowns. First, author Dr. Daniel Rudman remained adamant until his death that his study had no implications for anti-aging. In 2003, the NEJM published an editorial lashing out at the anti-aging industry for citing Rudman’s study so prominently in their advertising. “If people are induced to buy a ‘human growth hormone releaser’ on the basis of research published in the Journal, they are being misled,” the editorial stated.”
Does that sound like a sane design for ANY trial? Namely, the main intervention is actually known to cause the very things the trial hopes it will prevent? Of course not. And in their infinite wisdom (or wickedness) what did the study authors do to combat these effects of HGH? They added DHEA and metformin to “balance” the diabetogenic and pro-aging effects of HGH. But wait, it gets better. The study itself states that actually it is DHEA that is known for its anti-aging effects.
“…DHEA has many effects, in both men and women, that oppose deleterious effects of normal aging (Cappola et al., 2009; Forti et al., 2012; Shufelt et al., 2010; Weiss et al., 2011).”
So, how can we be sure that the reversal of biological aging seen in this trial was due to HGH and not the DHEA that was added for “balance”? We can’t, of course, and I highly doubt a trial design like this can happen by accident. The most likely explanation IMO is that the trial was purposefully designed to mask the anti-aging effects of DHEA and ascribe them to HGH – a hormone that numerous studies have shown is associated with every major chronic denegerative condition afflicting people over 50. Why do I suspect malice where stupidity would suffice? Well, it is this statement from the study:
“…Neither DHEA (Riley, Fitzmaurice, & Regelson, 1990) nor metformin are known to have any thymotrophic effects of their own.”
Just…wow! I simply can’t accept that a scientist working on thymus aging can be that ignorant or incapable of simple searches on PubMed. As often studied in introductory endocrinology, DHEA is one of the endogenous anti-glucocorticoid steroids (others including pregnenolone, progesterone, testosterone, DHT, etc) and has well-known effects on reversing thymus involution caused by aging and/or excessive glucocorticoid exposure. In fact, there is a study that performed the exact same experiment as the human study discussed in this thread and found that a physiological DHEA dose (equivalent to about 0.15mg/kg daily for a human) fully reversed immune system aging. Not partially, as in the human study above, but fully!
It is not just one study, there is a long list of publications discussing the immunotropic effects of DHEA in virtually every animal model known, and humans as well. Below is just a small subset of this list, which specifically points out the direct regenerative effects of DHEA on the immune system.
https://www.ncbi.nlm.nih.gov/pubmed/2141095
https://www.ncbi.nlm.nih.gov/pubmed/10718333
https://www.ncbi.nlm.nih.gov/pubmed/18461094
https://www.ncbi.nlm.nih.gov/pubmed/1835439
https://link.springer.com/article/10.1007%2FBF00925945
https://www.ncbi.nlm.nih.gov/pubmed/24022868
https://www.endocrine-abstracts.org/ea/0013/ea0013p164
https://jasn.asnjournals.org/content/19/1/92
And not to be outdone, the authors ensured that any positive effects of DHEA are handicapped from the get go. How did they achieve that? By administering a massive, unphysiological dose of 50mg DHEA daily. Physiological doses of DHEA are in the 10mg-15mg range. Multiple human studies have demonstrated that anything more than that quickly turns into estrogen, and of course that is what happened in this trial as well as confirmed by the development of gynecomastia (gyno) in one of the subjects.
“…Side effects included arthralgias (2 cases), anxiety (1 case), carpal tunnel syndrome (1 case), fluid retention (1 case), mild gynecomastia (1 case), and muscle soreness (1 case). One trial volunteer was removed from the study after approximately one month due to self‐reported bradycardia, which preceded the trial, and belated admission of a strong familial history of cancer.”
Why is the conversion of high doses DHEA into estrogen problematic? Because there is strong evidence that estrogen (together with cortisol) may be the primary causes of thymus involution seen with aging. Conversely, as demonstrated by the study below, inhibiting estrogen synthesis and/or effects has been shown to reverse thymus involution seen with aging. So, by giving such a large dose of DHEA the study authors (willingly or not) ensured that DHEA’s anti-aging effects would be severely handicapped.
https://www.sciencedirect.com/science/article/pii/0192056192901152
I am sorry, but nobody can be that ignorant, especially when deciding to include a chemical like DHEA in their study. A trivial search on PubMed would have turned up all of the above and a ton of additional evidence for the thymotrophic effects of DHEA, as well as its pro-estrogenic effects when administered in pharmacological (high) doses. So, why would a group of scientists design such a deliberately handicapped and bizarre trial? Well, by virtue of this design, the claim to fame goes to a patented, expensive and available-by-injection-only drug (HGH) instead of the humble, cheap, OTC anti-aging (when used in proper doses) chemical DHEA. I can already see Big Pharma arming its sales agents with the results of this human trial and sending them to doctors’ offices all over the country to push/market/sell various HGH preparations. A very similar tactic was used in recent clinical trials showing testosterone (T) injections stopping terminal prostate cancer in its tracks.
Cancer Paradox – Testosterone Injections Combat Lethal Prostate Cancer
Remember folks, according to the FDA androgens like T and DHT are supposed to cause prostate cancer, not cure it! In those trials, instead of ascribing the benefit of stopping the cancer to T, the benefit was ascribed to the co-administered “chemical castration” agent leuprolide. Why didn’t the leuprolide save the millions of other men (with metastatic prostate cancer) who got treated with it, but without the additional testosterone!? What would be the rationale of administering a “chemical castration” agent together with the very hormone the castration agent is supposed to block the synthesis of!? Only one reason, really. It is a desperate attempt to salvage the idiotic theory that androgens cause prostate cancer. This travesty is possible only because the public health authorities like the FDA have the power to ascribe benefits (or harm) from treatment to whatever chemical they choose. Whether that makes absolutely no sense, contradicts the evidence, is a potential conflict of interest (even fraud??), etc is immaterial. As we are told every day by mainstream media, we need medical degrees to be LICENSED/PERMITTED to even surmise we are being scammed. Simply put, we are NOT LICENSED to think for ourselves when it comes to our own health. This way people will obediently accept their “treatment” and simultaneously continue to be duped too so that they keep paying an arm and a leg for a system that quite openly kills them.
The bizarre design of the trial does not stop with HGH and abnormally high DHEA dosing. Same goes for metformin. It has become the darling chemical of the “official” (read: run by Big Pharma) anti-aging industry and multiple clinical trials with it are currently in progress with the hopes that it can reverse aging, treat/prevent cancer, dementias, Parkinson Disease (PD), osteoporosis, immune system aging, etc. None of those trials have shown an actual cure or reversal of aging. On top of that, now we have evidence that mitochondrial toxins like metformin raise lactic acid and cause systemic metabolic acidosis, which can directly CAUSE cancer. Remember, the Warburg “Effect” (lactic acidosis) is now acknowledged by even mainstream medicine to also be a cause of cancer.
Again, call me paranoid but IMHO the combination of all the above evidence makes it highly unlikely that such bizarre trial design occurred by accident. An honest, well-read, first-year medical student could have designed a more sane trial for reversing aging and would have likely achieved strikingly better results. How? Well, let’s start with one of the trial ingredients – DHEA. As the trial itself states, DHEA has known, potent, anti-aging effects. Those anti-aging effects include specifically reversing thymus involution/atrophy as per the studies I posted earlier in the thread. However, in order to reap the benefits of DHEA without its risks, we need to limit its propensity for conversion into estrogen. This is easily achievable by ensuring that DHEA is used in physiological doses, which for most adults span the range of 10mg-15mg daily. However, even 10mg single doses of DHEA have been shown to elevate estrogen when used for long periods of time, as anti-aging trials often require. There is evidence suggesting that individual doses of DHEA not exceeding 5mg raise systemic DHEA/S levels without raising estrogen levels. Thus, reaping the benefits of DHEA without its risks may be as simple as taking 5mg DHEA with each meal. For those still doubting the immuno-regenerating effects of DHEA (when used wisely) here is a human study showing administration of only DHEA was enough to re-activate the immune system in aged males.
https://www.ncbi.nlm.nih.gov/pubmed/9008662
Now, can we do better? Yes, yes we can! As I mentioned earlier, DHEA is one of several endogenous glucocorticoid antagonists. Such antagonists typically have thymotrophic effects, however such antagonists that are also strong androgens (ie. T, DHT, etc) can have detrimental effects on the thymus due to the activity on the androgen receptor (AR). So, in order to potentiate the anti-aging effects of DHEA on the thymus we need to combine it with an agent that is also a glucocorticoid antagonist yet does not cause thymus atrophy. Furthermore, it would be even more beneficial if the additional agent/chemical has anti-estrogenic effects as per the study I mentioned above showing that antiestrogenic agents can fully regenerate the thymus atrophied from aging. As many of my readers have already guessed, such remarkable agent/chemical already exists and its name is progesterone! The study below demonstrates the powerful thymotrophic effects of progesterone if used at the proper dosage.
https://cancerres.aacrjournals.org/content/canres/12/3/206.full.pdf
“…Of the steroids used, progesterone was the only one which produced a significant increase in the size of the thymus. All other compounds produced decreases of various degrees. The most effective steroids in this respect were cortisone, 11-dehydrocorticosterone, and testosterone. ACTH, cortisone, and 11-dehydrocorticosterone produced intense lymph node involution. Testosterone, the estrogens, and Reichstem’s Compound L all produced increased size of the lymph nodes.”
https://www.sciencedirect.com/science/article/pii/0022473179902504
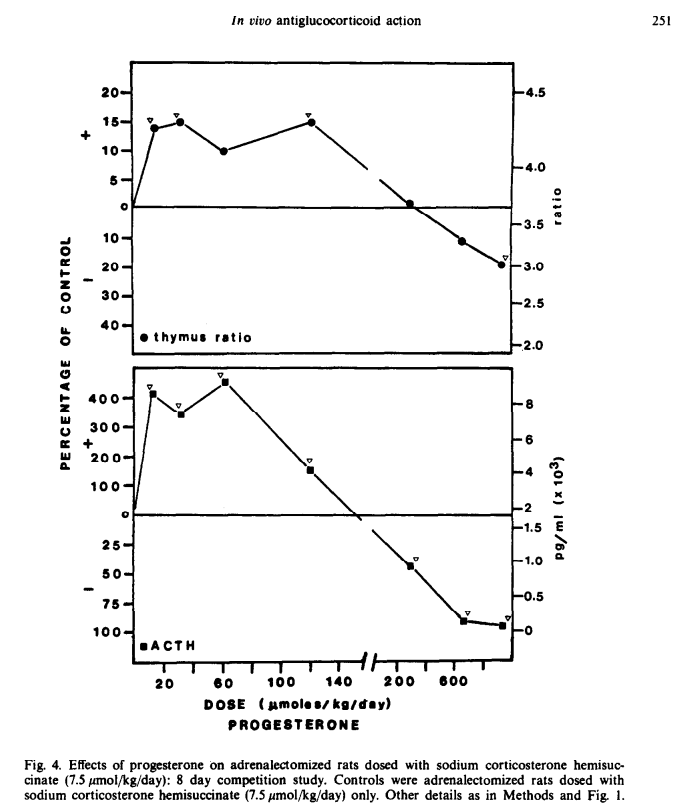
As readers can see from the study screenshot above, the optimal in-vivo dosage of progesterone for restoring thymus size/weight is in the range of 20 µmol/kg – 30 µmol/kg bodyweight daily. That corresponds roughly to a human dose of about 1 mg/kg daily. Higher progesterone doses did NOT have stronger thymotrophic effects and at doses of 200 µmol/kg (corresponding to doses about 10mg/kg for a human) daily or higher progesterone actually had detrimental effects on the thymus. So, in this case the expression “the dose makes the poison” rings quite true. Thus, for an adult weighing 75kg, the optimal daily progesterone dose would be about 75mg. This total daily dosage can be taken as a single dose or split into multiple smaller ones and still have the desired effect. However, it is well-known that when progesterone and DHEA are administered together progesterone has more potent effects of blocking DHEA’s propensity to convert into estrogen than when the two are administered at different times. Thus, considering the optimal regimen for DHEA is to use no more than 5mg per dose several times daily it makes sense to split that 75mg progesterone dose into as many doses as those of DHEA the person is taking daily and administer the two steroids together. For example, if a person is taking 5mg DHEA x 3 daily then they could split their 75mg progesterone dose into three doses of 25mg each and take 25mg progesterone with each dose of 5mg DHEA.
There is another caveat. The study with progesterone and thymus regeneration used a subcutaneous administration for the steroid, which ensures close to 100% bioavailability. Most progesterone products for humans (e.g. Prometrium) are designed for oral use and do not achieve 100% bioavailability. In fact, for most of those oral products the bioavailability is around 15%. So, if somebody is using an oral product like Prometrium then they would need to take a dosage that is 6-7 higher than the 1mg/kg administered subcutaneously. The good news is that when progesterone is dissolved in tocopherols/oil mixture its oral bioavailability is close to 100%. Similarly, when progesterone is dissolved in alcohol/fat combination and applied topically, its absorption is also quite high. More specifically, when either formulation is administered topically in the navel area, systemic bioavailability / absorption rivals IV route and application on other skin areas still achieves at least 50% systemic absorption of the administered dose.
Navel application/absorption rivals intravenous route, other skin routes not far behind
We already sell a product containing a progesterone/DHEA combination called CortiNon. Currently, it contains progesterone:DHEA in a ratio of 3:1, however we will soon be releasing a version where the progesterone:DHEA ratio will be raised to 8:1. That higher ratio product should provide progesterone and DHEA in such amounts as to match the known thymotrophic effects of both seen in the studies above (and hopefully even providing s synergistic effect than either one on its own), while minimizing the propensity of DHEA to convert into estrogen and thus harm the thymus.
That’s all folks. Apparently, the knowledge to reverse human aging using OTC ingredients is out there and has been laying hidden in plain sight for decades. Many of those studies demonstrating anti-aging, thymotrophic, pro-immune effects of progesterone/DHEA were published in the early 20th century. The fact that they have not gotten more publicity and have not been used to engineer a safe, effective anti-aging intervention is IMO nothing short of criminal negligence on behalf of the medical/pharma industry. I strongly encourage my readers to email the lead author of the TRIIM anti-aging trial (Gregory Fahy, fahy@interveneimmune.com) and ask why the decades-old published evidence on the possibility of safely reversing human aging with progesterone/DHEA has been ignored (or maybe concealed) for so long. Better yet, please demand answers as to why the TRIIM trial was designed in such a bizarre, unsafe, and openly biased manner. Namely, designed in order to ignore/handicap the known anti-aging effects of OTC chemicals like DHEA while simultaneously ascribing any demonstrated benefit to dangerous (but patented and profitable) interventions such as HGH (or even metformin) that the authors themselves state have pro-aging effects on thymus and immune system. If you get any answers, please send them over. I promise, I will publish them here.